21st Century Health Care Service Delivery
The Windsor Hospitals System Plan replaces all hospital services in the city core with urgent care and non-acute outpatient services.
Key Health Care Services that will be Lost from the City Centre:
The Windsor Hospitals System Plan replaces all hospital services in the city core with urgent care and non-acute outpatient services.
Key Health Care Services that will be Lost from the City Centre:
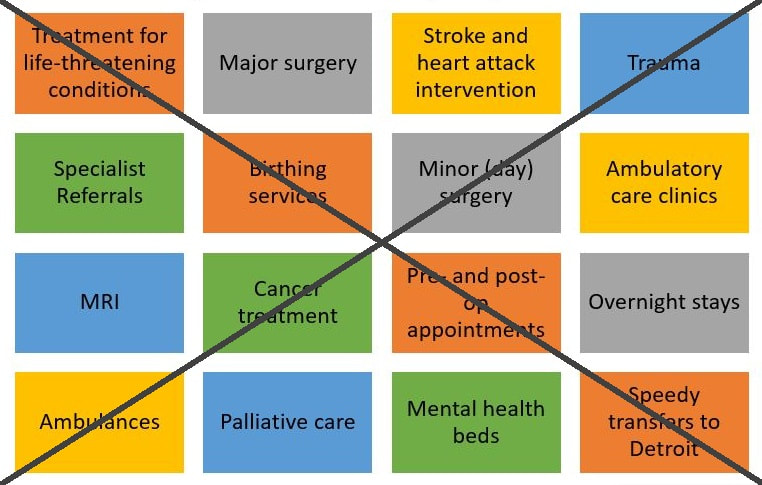
It is true that health care service delivery has experienced a major shift from inpatient to outpatient care. In the past two decades, hospital stays have fallen dramatically for many operative procedures.
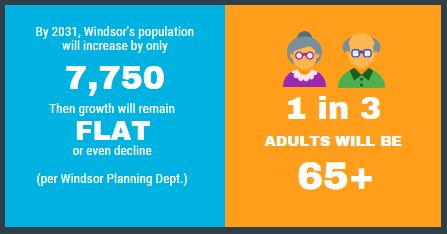
However, Windsor’s rapidly aging 21st century population has more complex medical conditions than ever before, leading to the need for a more extensive array of services than those planned to replace hospital services in Windsor’s city core.
Urgent Care is for less serious conditions
Urgent Care is not intended for life-threatening or complex conditions. It will not be available 24/7. The city’s lowest-income wards are home to the greatest number of people who do not drive. For tens of thousands of urban residents dependent on active transportation to get around, the planned hospital site will be considerably less accessible.
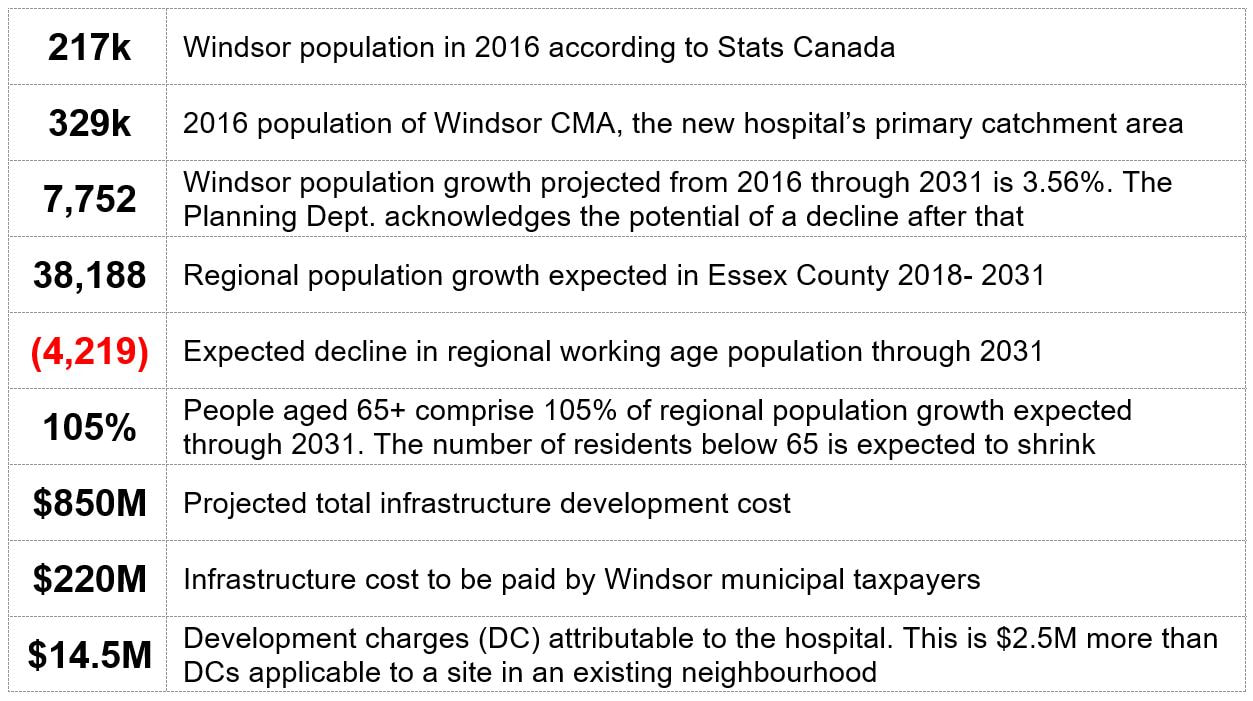
Key Numbers
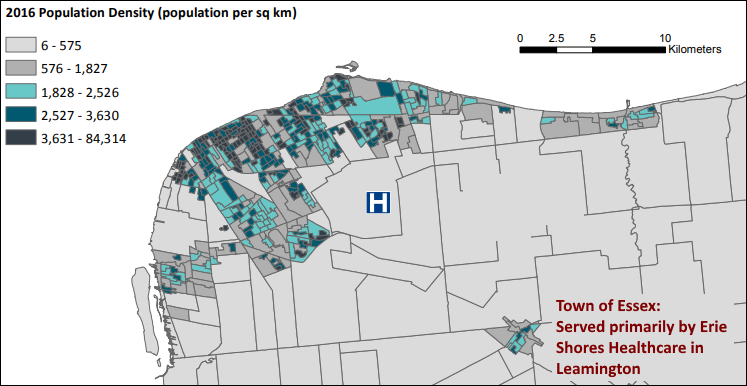
The greenfield hospital location is farthest from the Windsor CMA’s greatest population density:
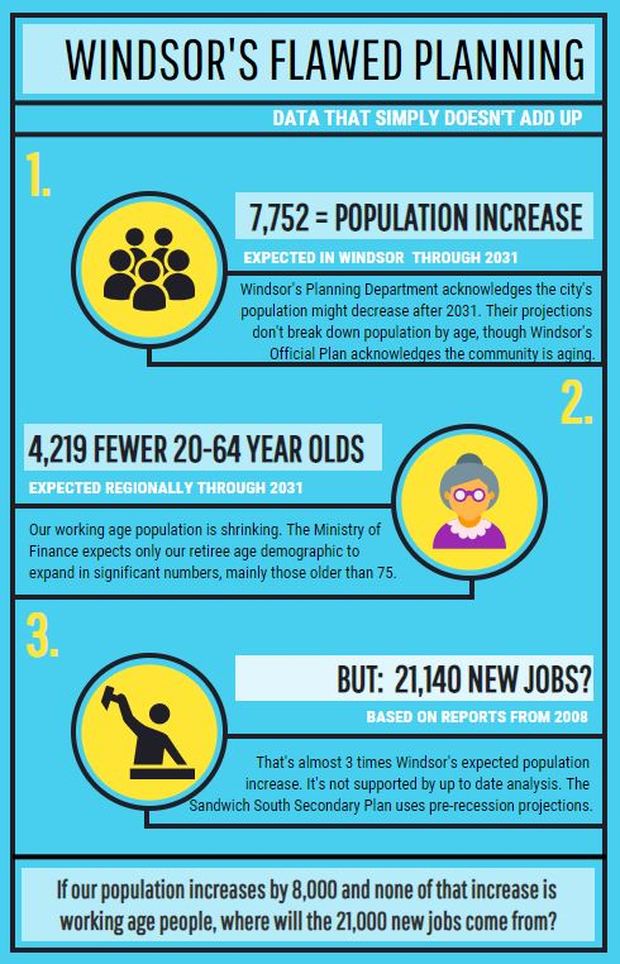
Flawed Data: Numbers That Don’t Add Up
The Ministry of Finance expects the regional supply of working age residents to decline over the next 13 years through 2031. Without growth among 20-64 year olds, there is no reason to expect significant employment expansion.
Employment growth of 21,140 jobs is based on obsolete population projections for Windsor:
The Ministry of Finance expects the regional supply of working age residents to decline over the next 13 years through 2031. Without growth among 20-64 year olds, there is no reason to expect significant employment expansion.
Employment growth of 21,140 jobs is based on obsolete population projections for Windsor:
- The employment land needs calculation is based on a 2008 study by EDP Consultants.
- They drew on 1996 and 2001 Census data and a 2008 Lapointe Consultants report.
The new hospital location is likely to result in greater capital and operational costs for services like road maintenance, EMS and public transportation.
Windsor’s infrastructure will be even more challenging to maintain than currently in view of stalled (or anticipated negative) population growth, as well as a rapidly aging and declining working age population.
Windsor’s infrastructure will be even more challenging to maintain than currently in view of stalled (or anticipated negative) population growth, as well as a rapidly aging and declining working age population.
Data that Backs Up the Infographic
Windsor’s Planning Department projects population growth of 7,751 through 2031
Windsor’s Planning Department projects population growth of 7,751 through 2031
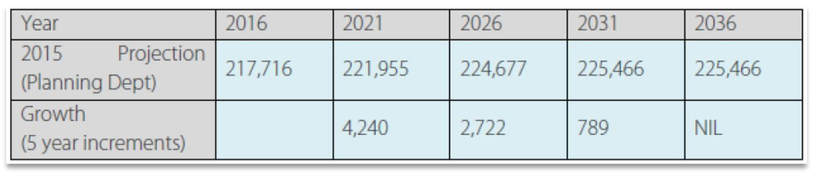
Source: Pg.18 of bit.ly/CAMPP_council
Yet, Altus Consulting, on behalf of the City of Windsor, inexplicably stands by an employment land needs forecast to accommodate 21,140 new jobs for Windsor residents. Of note:
Yet, Altus Consulting, on behalf of the City of Windsor, inexplicably stands by an employment land needs forecast to accommodate 21,140 new jobs for Windsor residents. Of note:
- 4,545 new manufacturing jobs, at a time of rapid loss of employment to automation
- 4,460 additional institutional jobs
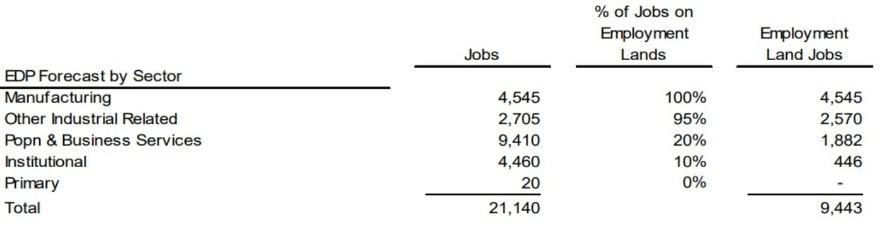
Source: Pg. 265 of bit.ly/CAMPP_altus
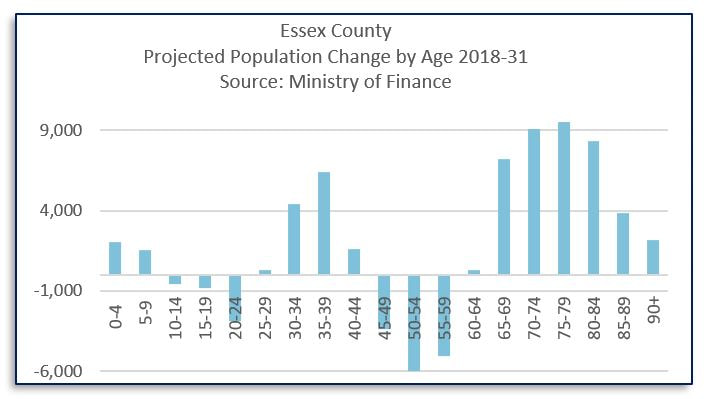
Windsor does not break down its projections by age, but regional projections from Ontario’s Ministry of Finance show:
- Population loss: expected among those younger than 65, in particular, the 45-59 age group
- Population growth: overwhelmingly concentrated among those of retirement age and older

Malfeasance?
Alteration of Consulting Engineer’s Figures
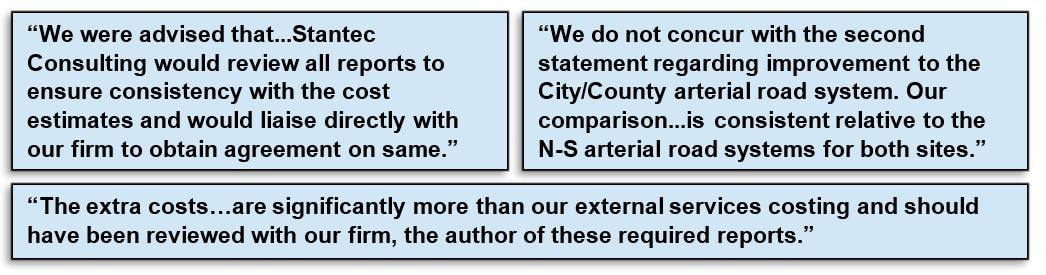
Significant taxpayer-funded costs were concealed from public scrutiny by altering the Consulting Engineer’s calculations after he submitted his figures, and by excluding known costs from the site evaluation.
Mr. Spencer, who is not in agreement with the substance of these alterations, wrote a letter that can be read in full at this link.
The following excerpts demonstrate the seriousness of his complaint:
Alteration of Consulting Engineer’s Figures
Significant taxpayer-funded costs were concealed from public scrutiny by altering the Consulting Engineer’s calculations after he submitted his figures, and by excluding known costs from the site evaluation.
- Phase 1 site selection favoured GEM, an infill site requiring only minor site infrastructure and no additional road construction
- Phase 2 eliminated GEM in favour of the County Road 42 site, on the basis of a $1.8M higher land acquisition cost differential. This was achieved by making significant changes to the figures submitted by Rick Spencer (the Consulting Engineer for both shortlisted sites), without consultation with him. Without these material alterations, the GEM site would have remained in first place
- External development costs, including upgrades to access routes, were excluded from the evaluation
Mr. Spencer, who is not in agreement with the substance of these alterations, wrote a letter that can be read in full at this link.
The following excerpts demonstrate the seriousness of his complaint:
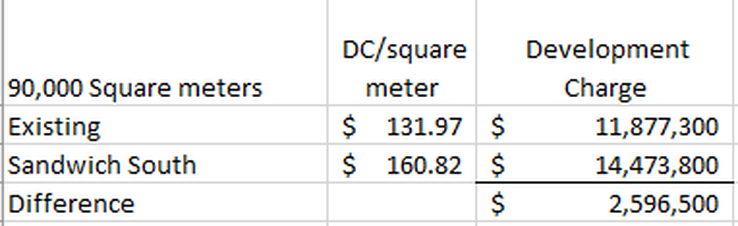
Development Charges (“DCs”)
DCs allocate the true cost of infrastructure investments where they are incurred. They were excluded from the ranking of the shortlisted sites. In this way the greenfield site was artificially made to appear more cost-effective than a fully serviced infill site. Had DCs been considered, the GEM site would have remained in first place. DCs would have reversed the $1.8M land cost differential that put the County Road 42 site in the winning position in Phase 2.
DCs allocate the true cost of infrastructure investments where they are incurred. They were excluded from the ranking of the shortlisted sites. In this way the greenfield site was artificially made to appear more cost-effective than a fully serviced infill site. Had DCs been considered, the GEM site would have remained in first place. DCs would have reversed the $1.8M land cost differential that put the County Road 42 site in the winning position in Phase 2.
Fairness Advisor’s Limited Mandate
The appointment of a Fairness Advisor to oversee just a portion of the site selection process created a false appearance of integrity. His mandate excluded evaluation of site selection criteria:
The appointment of a Fairness Advisor to oversee just a portion of the site selection process created a false appearance of integrity. His mandate excluded evaluation of site selection criteria:

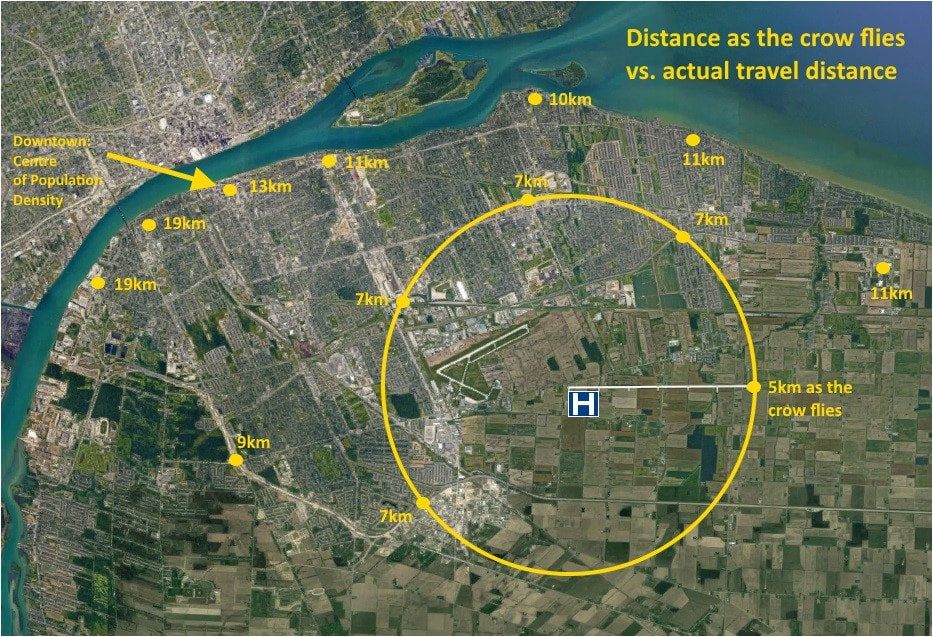
Accessibility Measured as the Crow Flies; Population Density Ignored
The site selection criteria used radius (rather than population density or travel distance) to evaluate accessibility
1. Proposed hospital location on County Rd 42, showing actual travel distances that greatly exceed the distance as the crow flies:
2. Actual travel distances to top-scoring GEM property, an infill site that is surrounded by residential neighbourhoods and served by public transit today:

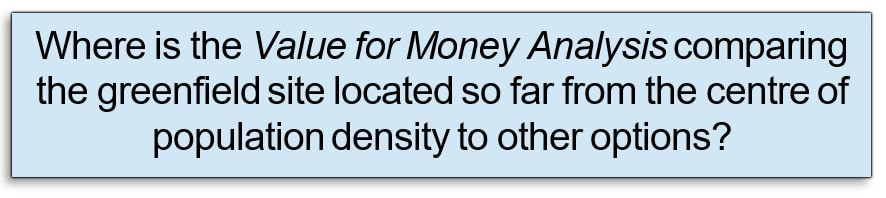
None of these Analyses have been Performed
Thorough analysis of the impacts of the County Road 42 hospital location is needed to ensure effective and cost-efficient planning
Demographics
Financial
How removing an acute care hospital will impact Windsor’s urban core
How health care professionals will be affected
Carbon Footprint
Ontario Planning Policy
Outdated Reports Used for Decision-Making
- Windsor population growth projection by age group
- Residential housing needs after factoring in planned downtown Community Improvement Plan (CIP) projects
- Places of Employment, using the same up to date population growth projections that were used to project residential housing needs
Financial
- Fiscal Impact Analysis of Sandwich South development to determine lifecycle cost recovery
- Updated Technical Building Assessment (last performed 2008)
How removing an acute care hospital will impact Windsor’s urban core
- Long term economic consequences of loss of 3-4,000 jobs from the city core
- Cost to expand service area and maintain public transportation network (currently not 24/7)
- EMS capital and operational needs resulting from increased travel distances from areas of social deprivation (a LHIN term) to the new hospital
- ER referrals for non-admitted patients to determine location & frequency of follow-up care
- Mental health ER usage and admissions after 10 p.m.
- Transit dependency and socio-economic factors affecting patient mobility
How health care professionals will be affected
- Survey of health care workers who live within walking distance of existing hospitals
- Survey of physicians to determine how many will have to move to the area around the new hospital (e.g. physicians and nurses with on-call responsibilities)
Carbon Footprint
- Environmental impact of a greenfield hospital on County Road 42
Ontario Planning Policy
- Impact of hospital location on aggregate vehicle trips and commute distances
- Barriers to access for seniors and persons with impaired mobility
Outdated Reports Used for Decision-Making
- Sandwich South Employment land needs calculation is based on 2008 EDP Consultants’ report, which drew on 1996 and 2001 Census data and a 2008 report by Lapointe Consultants
- Lauzon Parkway EA (Pg.110) (roads to be upgraded under the Sandwich South Secondary Plan), used 2006 Census data to project population growth of 30k through 2031 and is no longer valid
- Windsor Asset Management Plan and Strategy: current plan is dated 2013
- Brownfield Land Inventory: current strategy is dated 2012
- Official Plan: statutory 5 year review was last updated in 2013
Smoke and Mirrors
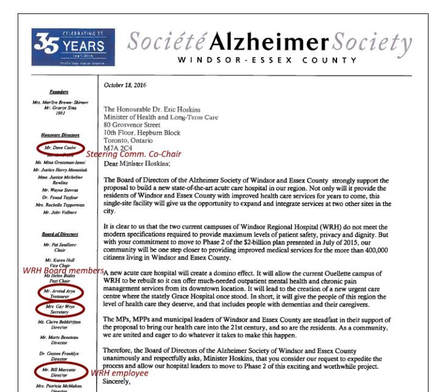
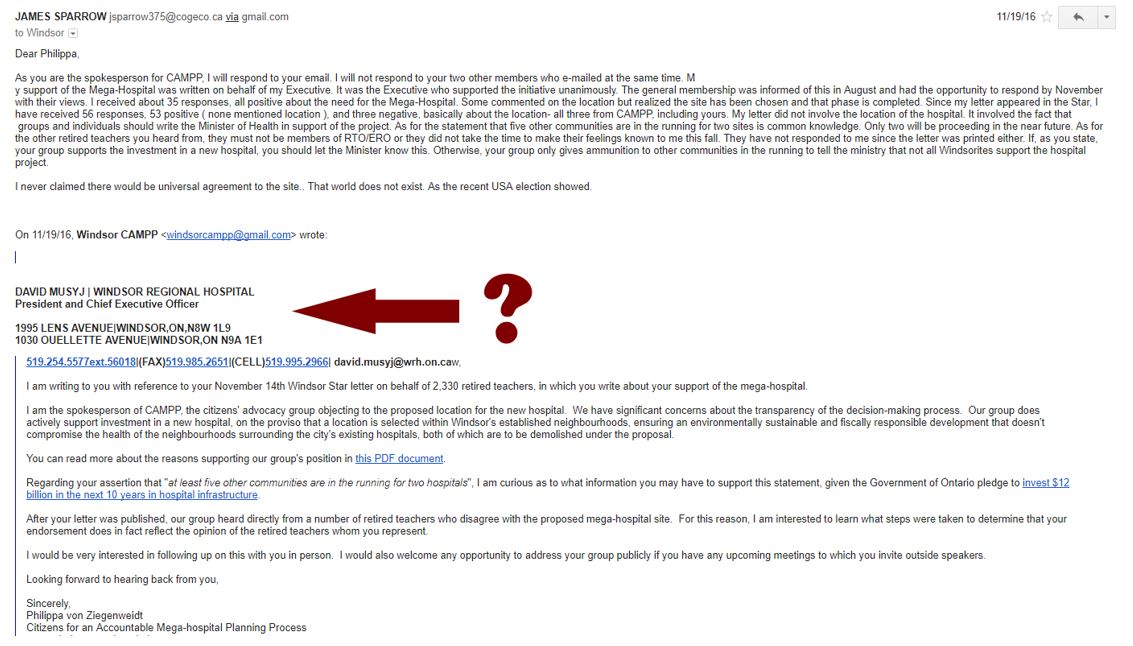
Letters of Support Obtained through Relationships of Influence
A complex web of Board and professional relationships influenced the letters used to demonstrate community support for this project.
Letters of Support Obtained through Relationships of Influence
A complex web of Board and professional relationships influenced the letters used to demonstrate community support for this project.
|
Many referred to the hospital without referencing its controversial location. Three examples of relationships that were closer than at first glance: 
|
|
Why was WRH CEO David Musyj coaching the Retired Teachers of Ontario?
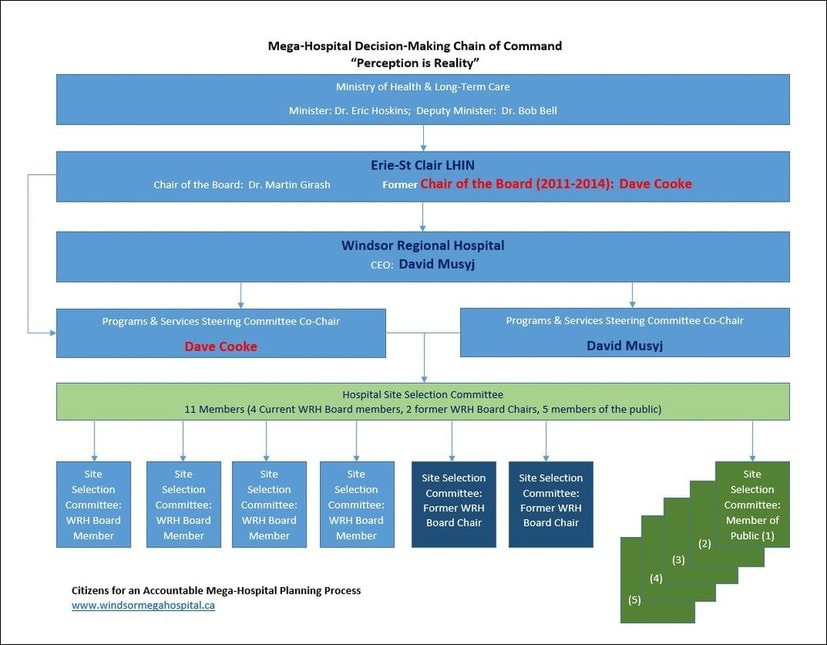
Opaque and Convoluted Decision Making Structure
According to the Erie St. Clair LHIN, location is Steering Committee’s responsibility
- Yet LHIN approval is a requirement for Ministry to proceed
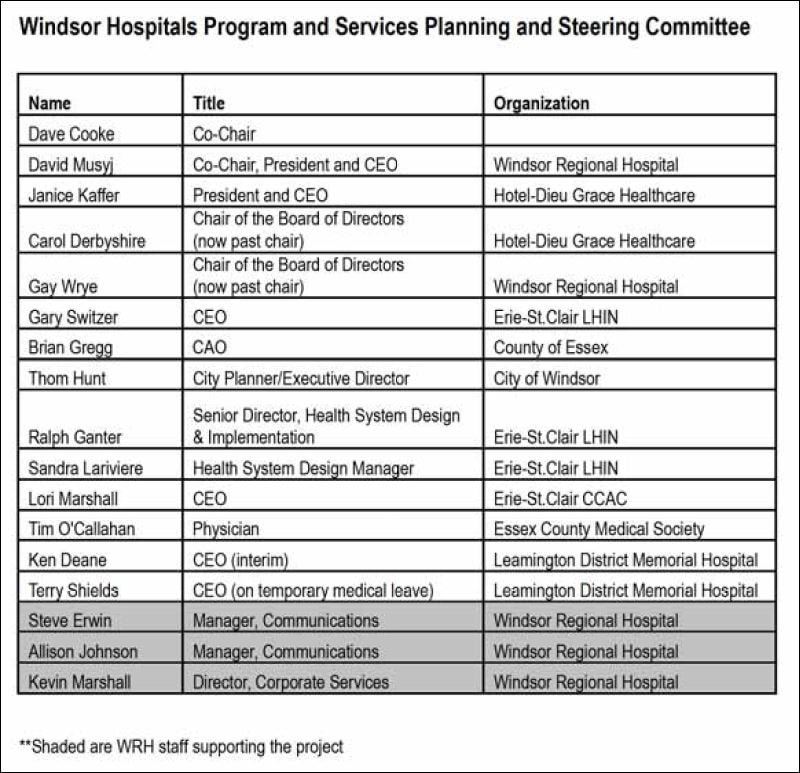
- Five Steering Committee members were Erie St. Clair LHIN employees
Steering Committee is accountable to WRH Board
- Majority on Site Selection Committee associated with WRH Board
- Site Selection Chair was also Chair of WRH Board at the time of the location decision (July 2015)
- WRH Board did not respond to CAMPP’s May 2017 letter outlining concerns
Erie St. Clair LHIN role
- Dave Cooke, Steering Committee Co-Chair, is former LHIN Board Chair
- Board meetings held in Chatham (82km from Windsor)
- Currently no Board members live in Windsor, although Windsor represents 1/3 of the Erie St. Clair LHIN population
- It took more than 12 months and many requests from CAMPP to get the LHIN to meet in Windsor (May 24, 2016)
- Only 3 residents were permitted to speak at this non-Town Hall meeting
- LHIN Board gave no subsequent response to CAMPP’s questions
- LHIN Chair Dr. Martin Girash claimed LHIN played no role in site selection
Mayor Dilkens claimed location was outside City’s purview (April 2016 levy meeting)
- Mayor Dilkens said location was already decided (August 2018 zoning meeting)
- However, plan includes a land swap between WRH and City of Windsor that has never been discussed at City Council, raising questions about valuation, due diligence and lines of responsibility for decision making.
The Decision Makers
The hospital project reached planning Stage 2 under former Minister of Health, Dr. Eric Hoskins. Ontario’s new Minister of Health, Christine Elliott, has not made any further announcements.
|
|
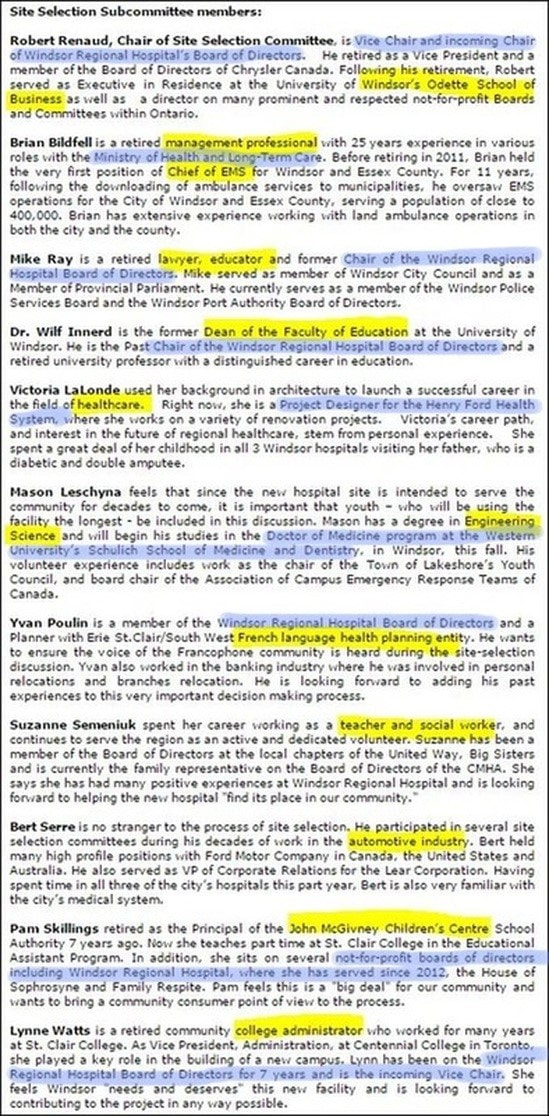
Site Selection Committee Controlled by WRH
- Four serve(d) on the Board of WRH, another 2 are former Chairs of the Board
- Only 3 are members of the public without apparent ties to WRH
Furthermore, none of the of 11 committee members has a planning background.
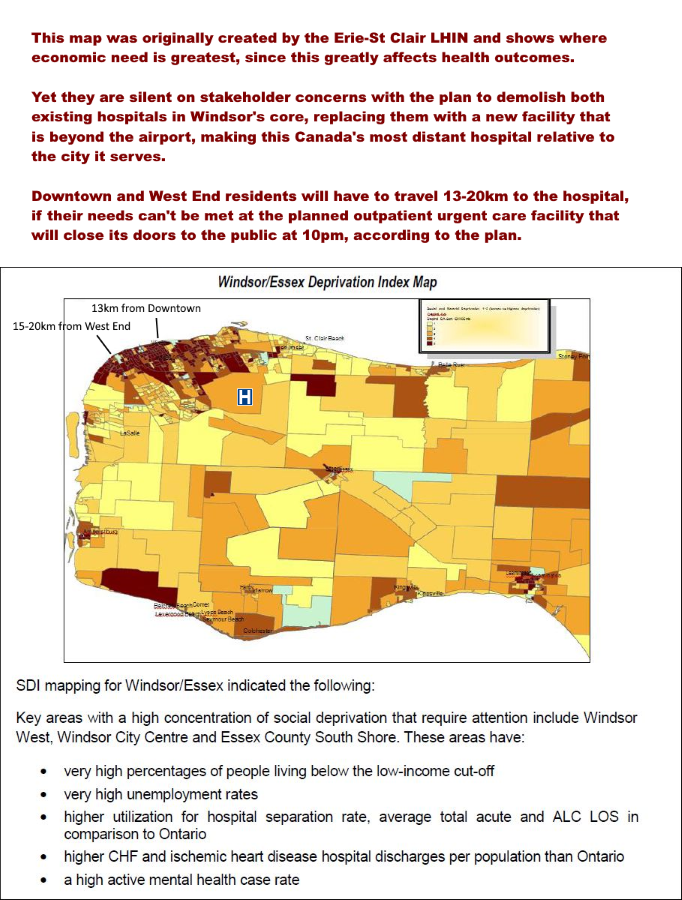
Social Deprivation in Hospital Use Ignored in Site Selection
- According to the Erie St. Clair LHIN, neighbourhoods with higher deprivation index scores have higher hospital utilization rates
- The County Road 42 site achieved an 80% site selection score for Proximity to EMS services (#15). The scoring description includes a requirement that travel times for emergency services to the hospital be less than current times. No data is available to justify this improbable score
600+ Bed Hospitals Cost More Money to Run
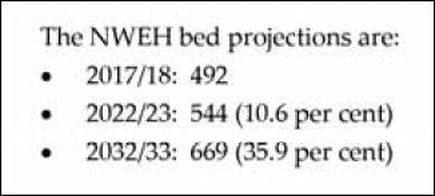
Projections show all of the region’s population growth among the senior population (the demographic group with the greatest hospitalization rates). Yet:
- The new hospital is to have the same number of beds (just under 500) on opening day that WRH has now
- The plan indicates a need for 669 beds, but not until 2032/33
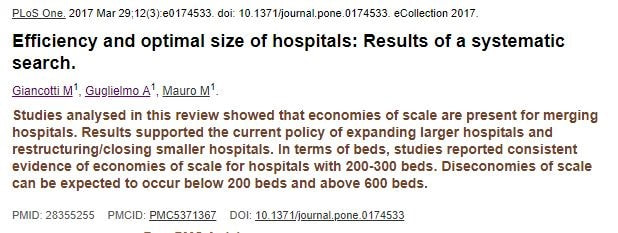
Optimal hospital size
Studies consistently report improved economies of scale for 200–300 bed hospitals:
- Dis-economies of scale can be anticipated below 200 and above 600 beds
- This contradicts the wisdom underlying Ontario’s decade-old mega-hospital construction trend
This is the conclusion found in this March 2017 metadata study:
Similarly, in Are bigger hospitals better?, the Health Evidence Network (a WHO member agency) concludes: “It is tempting to think that larger hospitals are more cost-effective than smaller ones because of the operation of economies of scale. However, the evidence does not back up this belief…The literature on hospital economies of scale suggests that they are fully realized in facilities of 100 to 200 beds…Research shows that they rarely result in lower costs or better patient outcomes.”
This should serve as a sober warning for decision-makers seeking the wisest and most cost-effective way to allocate scarce health care resources
Decision Makers Ignored Residents’ Concerns
|
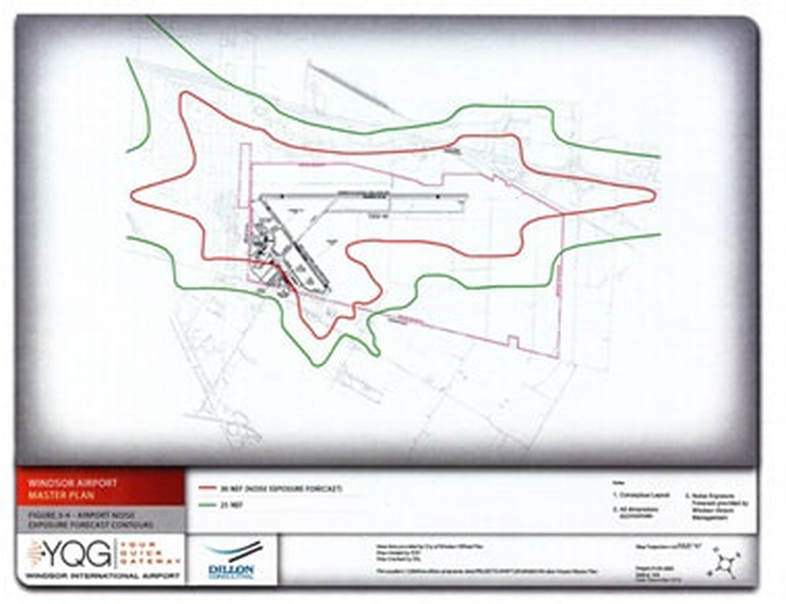
Many residents have unresolved concerns about the construction of the region’s only hospital close to Windsor Airport. For example:
|
|
Limitations on Future Expansion
- Height restrictions in the airport’s flight path will preclude future vertical expansion of the hospital
- Noise exposure forecast (NEF) contour restrictions close to the hospital site also preclude the possibility of future runway expansion
No Meaningful Community Consultation
The public’s concerns about the hospital location have never been addressed
- For four years Mayor Dilkens declined to meet with members of CAMPP about the community’s concerns, claiming he had no influence, even though the deal included a major municipal land swap.
- The meeting to proceed with the tax levy to pay the 10% local share of the hospital cost was squeezed at short notice into the agenda for the December 21, 2015 Council meeting. This was also the annual Budget meeting, already the longest meeting of the year. The Mayor stressed that the location of the hospital was not to be discussed.
First Nations Consultation under UNDRIP: There has been no meaningful consultation with First Nations
Emails invitations to a stakeholder meeting were sent to Caldwell and Walpole Island First Nations. Secondary Plan appendices indicate no response was received.

At the April 25, 2016 Windsor City Council meeting, a First Nations resident spoke about the requirement for meaningful consultation under UNDRIP obligations. However, no further efforts were made to engage First Nations.
Lack of Accurate Public Messaging: Many residents still incorrectly believe the new hospital is an additional facility
- Many refuse to believe the project involves the loss of both existing hospitals.
- Another prevalent misconception is that the new hospital will provide additional programs and services so residents will no longer have to travel to London or Toronto for specialized treatment. Several Windsor councillors even indicated they believed this to be true at the August 13, 2018 zoning meeting. Without significant population growth and operating resources, this is an unrealistic dream.
- The community has consistently expressed significant concerns regarding the hospital location at meetings, in person, in letters, on social media, through billboards and with thousands of highly visible lawn signs.
- Meanwhile, the Steering Committee Co-Chairs consistently marginalized all expressions of concern, referring to those in opposition to the plan as a small group putting the success of the project at risk.
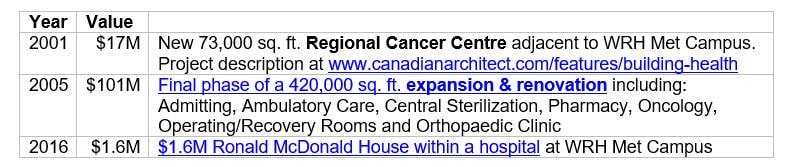
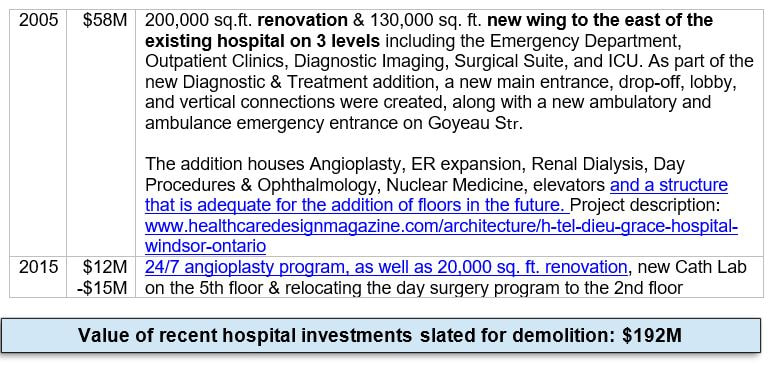
Demolition of 21st Century Capital Investments
1. Windsor Regional Hospital Met Campus – to be demolished:
2. Windsor Regional Hospital Ouellette Campus – to be demolished:
3. HDGH Tayfour Campus

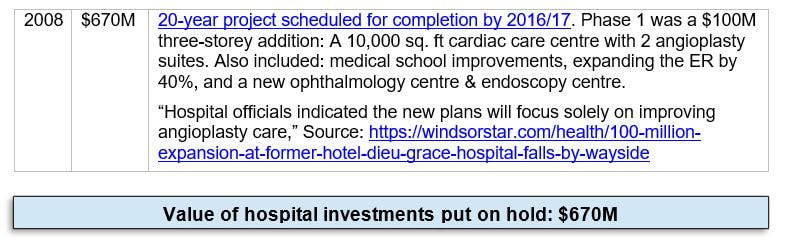
4. Windsor Regional Hospital Ouellette Campus – put on hold:
Time Line
Date Details
Jun 2009 Master plan, with greenfield site and demolition of Windsor Regional Hospital including Cancer Centre (2001) identified as preferred option
Nov 30, 2012 Windsor Hospitals Study Final Report released
Nov 23, 2013 Stage 1A announced
May 7, 2014 Public invited to apply for 4 of 10 positions on Site Selection Committee. Deadline May 16th.
May 20, 2014 Site Selection Committee announced
May 25, 2014 Survey: Public invited to rank a predetermined set of site selection criteria
Jun 11, 2014 Site Selection criteria announced
Jul 23, 2014 Land offers accepted
Jul 16, 2015 County Road 42 site announcement
Nov 11, 2015 The only downtown public meeting (hosted by DWBIA)
Dec 21, 2015 Windsor City Council Levy Meeting (Note also: “Levy, not Location”)
Dec 22, 2015 Lawsuit launched against WRH by GEM Properties (later dropped)
Jan 7, 2016 News release on site selection following CAMPP FOI request
Apr 20, 2016 County Council approves levy share
Apr 25, 2016 Windsor Council approves levy share
May 24, 2016 Erie St. Clair Board Meeting in Windsor (set of questions presented by CAMPP to the Board)
Sep 7, 2016 Public information meeting on Secondary Plan convened by Stantec (official response submitted by CAMPP)
Jul 5, 2017 Public meeting convened by MHBC Consultants (official response submitted by CAMPP)
Dec 1, 2017 Dr. Hoskins announces Stage 2: Adds that the re-use of Ouellette Campus instead of Grace Site will be investigated
Feb 2, 2018 MHBC Background Plan submitted to City of Windsor
Aug 13, 2018 Combined Planning and Council meeting to approve Secondary Plan Amendment and hospital zoning
SEP 17, 2018 Council adoption of Secondary Plan Amendment and hospital zoning by-laws
Jun 2009 Master plan, with greenfield site and demolition of Windsor Regional Hospital including Cancer Centre (2001) identified as preferred option
Nov 30, 2012 Windsor Hospitals Study Final Report released
Nov 23, 2013 Stage 1A announced
May 7, 2014 Public invited to apply for 4 of 10 positions on Site Selection Committee. Deadline May 16th.
May 20, 2014 Site Selection Committee announced
May 25, 2014 Survey: Public invited to rank a predetermined set of site selection criteria
Jun 11, 2014 Site Selection criteria announced
Jul 23, 2014 Land offers accepted
Jul 16, 2015 County Road 42 site announcement
Nov 11, 2015 The only downtown public meeting (hosted by DWBIA)
Dec 21, 2015 Windsor City Council Levy Meeting (Note also: “Levy, not Location”)
Dec 22, 2015 Lawsuit launched against WRH by GEM Properties (later dropped)
Jan 7, 2016 News release on site selection following CAMPP FOI request
Apr 20, 2016 County Council approves levy share
Apr 25, 2016 Windsor Council approves levy share
May 24, 2016 Erie St. Clair Board Meeting in Windsor (set of questions presented by CAMPP to the Board)
Sep 7, 2016 Public information meeting on Secondary Plan convened by Stantec (official response submitted by CAMPP)
Jul 5, 2017 Public meeting convened by MHBC Consultants (official response submitted by CAMPP)
Dec 1, 2017 Dr. Hoskins announces Stage 2: Adds that the re-use of Ouellette Campus instead of Grace Site will be investigated
Feb 2, 2018 MHBC Background Plan submitted to City of Windsor
Aug 13, 2018 Combined Planning and Council meeting to approve Secondary Plan Amendment and hospital zoning
SEP 17, 2018 Council adoption of Secondary Plan Amendment and hospital zoning by-laws
